|
This case presents a 62 year old woman with a complaint of pulsatile tinnitus RE for several months. The pulsations are noted intermittently throughout the day but particularly apparent when she lays down. There is no associated hearing loss or otalgia. There is a history of bilateral hearing loss, middle ear infections, central perforation AD and occasional vertigo. The vestibular complaints had been present for over 20 years with a past diagnosis of vestibular Menieres. The central perforation had been surgically repaired in 1973. She had worn a hearing aid many years ago but discontinued its use.
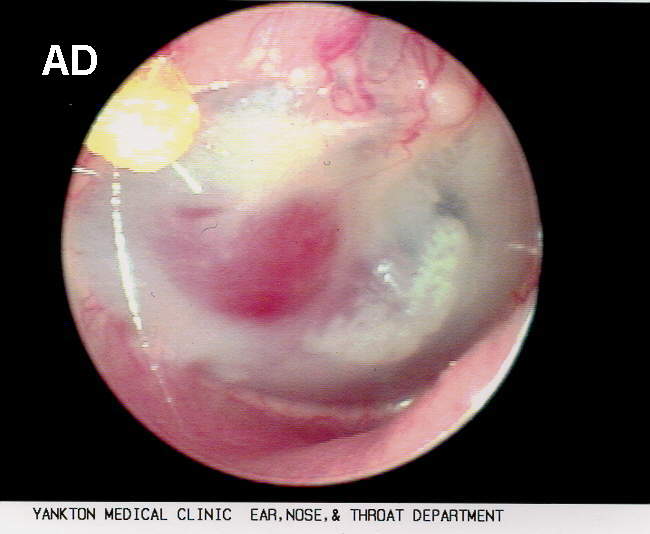
Physical exam revealed a heavily sclerotic right TM with a reddish mass slightly bulging from the central portion of the TM. It appeared to arise from the substance of the TM or perhaps behind the TM. While observing the mass with the VO subtle but discernible pulsations of the mass were apparent.
glomus tympanicum, AD; 62Y.F.[click to enlarge]
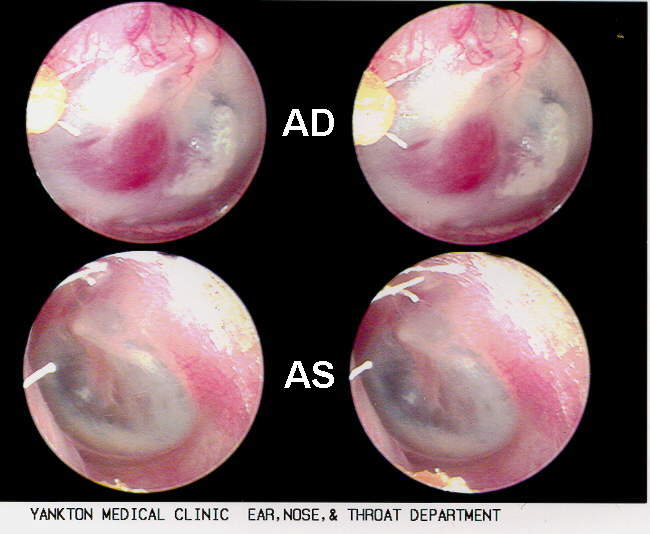
Same case, AD / AS comparison [click to enlarge]
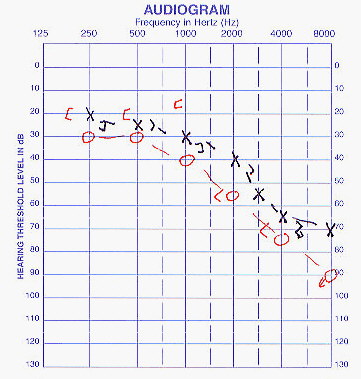
The audiogram showed a mild to moderately-severe sloping HL AU greater AD with small a/b gaps 250-1KHz in AD.
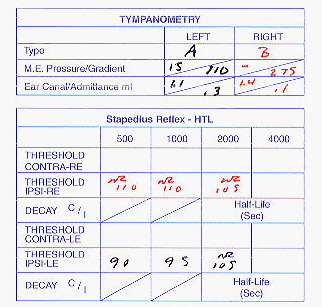
Tympanogram was Type B (flat) with absent ipsilateral reflexes. No pulsatile deviations in admittance were noted during tympanometry.
A high resolution CT of the inner ear and temporal bones showed a soft tissue mass localized to the hypotympanum. It occupied an area from the bony wall of the inner ear to the scutum and inferiorly to the floor of the tympanic cavity below the TM. It did not appear to be expansile or causing adjacent destruction of the middle ear. No involvement of the jugular foramen, mastoid air cells or other major vascular areas were noted.
Preoperative diagnosis was a glomus tympanicum or a small glomus jugulare. Other benign neoplasms or vascular anomalies were considered. The fact that the previous surgical report did not mention an aberrant vessel weighs against an anomalous blood vessel.
The patient was scheduled for excision of the middle ear mass by a transtympanic approach. When the middle ear was entered a reddish, lobulated mass was encountered filling the entire posterior two-thirds of the middle ear space, extending from about the level of the incus superiorly, anteriorly to the handle of the malleus, posteriorly into the sinus tympani region and inferiorly, down into the the hypotympanum. The frozen section confirmed the mass to be a middle ear paraganglioma or glomus tympanicum tumor.
Case contributed by Kevin Pons, M.S., FAAA; Yankton Medical Clinic; Yankton, SD
posted March 28, 1999
|