
This 28 year old male patient was diagnosed at the age of 6 as having a unilateral (AD) essentially conductive loss of hearing, mistakenly ascribed to ear infections in infancy. Figure 1 show a contemporary audiogram. Figure 2 presents tympanometry results.

In Figure 3, VO reveals an hypertrophic fused malleus / incus, AD. Both crura of the congenitally displaced stapes are visible through the TM. AS TM appears dull with a diminished light reflex and some squamous migration noted postero-superiorly.

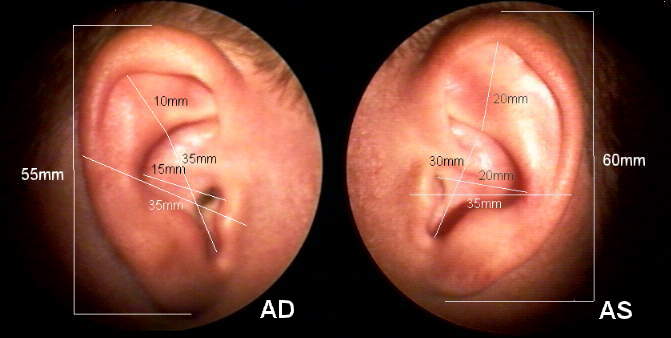
In figure 4 , VOM enables a direct comparison of the right and left pinna. Note the dimensional derangement especially in the area of the AD superior helix.
At the age of 18, the patient underwent an exploratory tympanotomy. A dehiscent, low hanging facial nerve necessitated termination of the procedure. A subjectively unsatisfactory trial experience with CIC amplification AD prompted the patient to reconsider the surgical option, for which he was given a referral. A reexploration of the AD middle ear was performed by a highly experienced otologic surgeon who returned the following report of findings:
Dear Roy, I have to report to you that because of the aberrant exposed and prolaped facial nerve, it was my best judgement not to proceed with the surgery. The loose facial nerve sagged down into the oval widow niche lying against the promontory completely obstructing any visualization of the oval window. In view of the normal hearing in the opposite ear and a possibility of injury to the facial nerve which could result in paralysis of the face, I decided to replace the eardrum and close the ear. I explained all this to the family and I know they appreciated the situation. .........
The patient will have periodic audiological follow-up evaluations with reconsideration of corrective amplification PRN.
© 1996 Roy F. Sullivan, Ph.D. (04/13/96)