Ear Impression-Taking in Ear Canals Surgically Altered by Modified Radical and Radical Mastoidectomy and Fenestration.Roy F. Sullivan, Ph.D. (posted 10/18/1995; revised 03/05/1999)
The most challenging ear impression-taking experience for the audiologist is that of an ear which has been surgically altered through intact wall mastoidectomy, modified radical mastoidectomy, radical mastoidectomy or fenestration, which included a mastoidectomy for exposure. The extensive iatrogenic undercut in the posterior bony canal must be carefully observed, then safely and effectively provided for in order to avoid impression material impaction. One wishes to achieve accurate dimensioning in the lateral cartilaginous canal with some extrapolated, linear extension into the medial canal area contiguous with the surgical canal defect. Demonstration by Video Otoscopy has been very helpful in securing the patient's full cooperation and understanding of the difficulties and limitations in fabricating an acoustic coupling for this type of ear. The VO images below represent the documentation of an impression-taking procedure in the right ear of a 69 year old female patient with bilateral modified radical mastoidectomies to be fitted binaurally with CLASS II full concha hearing aids. Candidates for corrective amplification in these post-surgical categories are invariably under the ongoing care of an ENT physician for cavity hygiene and maintenance. It is essential that the ear is free of cerumen and debris and that full ENT medical concurrence is obtained before proceeding with the impression-taking and hearing aid fitting. Figure 1 (19k) shows the VO view of the right ear canal which has undergone a classic Bondy-type modified radical mastoidectomy. The PVT in this ear is 4.5ml eq.  In Figure 2 (19k) we see a surgically enlarged meatal aperture in the background with #3 and #5 (Hal-Hen) cotton blocks and earlight tip in the foreground. Foam blocks do NOT provide adequate protection for this procedure.  Figure 3a (22k a+b) demonstrates placement of the large #5 cotton block into the posterior wall mastoid cavity. The anterior margin of the block should be visible. If not, a larger sterile cotton block should be hand-tied with button twist. The #3 cotton block is then inserted to protect the TM (3b). Size and placement of the multiple blocks will vary from case to case.  The author has found that monomer/polymer (powder and liquid) impression material is less likely to impact or tear than silicone. Figure 4 (21k) presents the resulting ethyl methacrylate impression with cotton blocks attached.  Contingent upon the acoustic coupling class of the fitting, in this case, CLASS II (vented), the impression should be detailed with a hand motor tool to ease severe undercuts. Figure 5 ( 23k) displays the impression pre- (a) and post-detailing (b). The laboratory should be informed that this is a surgically altered ear. 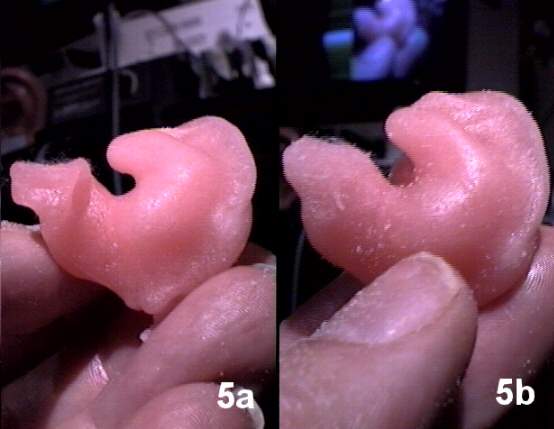 Figures 6a and 6b (25k) show the resulting full concha hearing aid in situ (a) and (b) in isolation to demonstrate the canal segment of the instrument which was both comfortable and feedback-free at time of fitting.  |